MK677 and Ipamorelin are both selective agonists of the ghrelin receptor. Ipamorelin is a peptide analogue of ghrelin whereas MK677 is an unusual molecule that doesn’t fit into any specific category (it isn’t a peptide). These two compounds, while affecting a similar receptor, have different properties and produce different biochemical results. Many people are interested in the differences between MK677 vs Ipamorelin. Below is a look at how these compounds differ as well as how they are alike.
MK677, also known as Ibuatmoren and Oratrope, is an orally active, non-peptide, selective agonist of the ghrelin receptor. MK677 shares no structural similarities with ghrelin and therefore no structural similarities with Ipamorelin. Research shows that MK677 increases the secretion of growth hormone (GH) and insulin-like growth factor-1 (IGF-1) without affecting cortisol levels. It is currently under investigation for the treatment of growth hormone deficiency, muscle wasting, bone wasting, and appetite stimulation. MK677 has a long half-life and once-daily dosing in most trial settings.
Ipamorelin is a peptide analogue of ghrelin that stimulates the secretion of GH. It is among the most selective of ghrelin analogs with research revealing no effect on ACTH, prolactin, follicle-stimulating hormone, luteinizing hormone, thyroid stimulating hormone, or cortisol levels. Ipamorelin has been investigated in the treatment of GH deficiency, muscle wasting, and post-surgical ileus. It has also been the subject of numerous clinical trials for its ability to increase bone strength and mineralization.
Molecular Weight: 528.7 g/mol
PubChem CID: 9939050
Synonyms: MK-0677, Oratrope, Ibutamoren
Source: PubChem
Molecular Formula: C38H49N9O5
Molecular Weight: 711.868 g/mol
PubChem CID: 9831659
Source: PubChem
It is interesting that MK677 and Ipamorelin are so different because the effects these compounds have at the ghrelin receptor are very similar. Both bind to the ghrelin/growth hormone secretagogue receptor to boost GH release. Both also maintain the normal, pulsatile patterns of GH fluctuation. They both also have high degrees of specificity and therefore very few side effects.
Oddly, the fact that MK677 isn’t a SARM is of massive benefit. SARMs usually impact natural androgen production and can lower testosterone production. They certainly have their place in the clinical setting, but SARMs must be carefully administered to avoid side effects. Neither MK677 nor Ipamorelin has this requirement. There is no evidence that either molecule needs to be cycled to prevent tachyphylaxis (a loss of efficacy usually due to the down regulation of receptors in the setting of high stimulation).
Overcoming somatopause is a hot research topic. Studies suggest that stabilizing the GH axis produces a number of benefits with age including enhanced immunity, increase muscle strength, and improve cognition. While body composition may not seem like an important consideration with age, it is actually critical to health and wellbeing. Increased muscle strength helps to prevent things like slips, trips, and falls that become more common with age. Additional evidence suggests that elevated GH levels can help to reduce cardiac risk as well by driving down fat levels and the associated increases in triglycerides and cholesterol levels that come with high body fat content. It is worth noting too that fat is a source of inflammation that has been linked to diabetes and other inflammatory diseases. There is good reason to believe that reduced fat mass can help to prevent diabetes and even conditions like rheumatoid arthritis[2]. Inflammation is also a component of cardiac disease, so reducing total body inflammation may be just one of several mechanisms by which elevated GH levels help to thwart heart disease.
Both MK677 and Ipamorelin are under study for their ability to halt or even reverse some aspects of somatopause. MK677 is of particular interest due to its ease of administration. Whereas Ipamorelin is only active when injected, MK677 is highly effective when taken by mouth.
MK677 significantly increases both bone deposition and resorption, leading to increased bone remodeling[3], [4]. This can, when properly controlled, lead to increased bone strength and resistance to fracture. Pairing MK677 with physical therapy leads to increased bone density and decreased risk of hip fracture in elderly individuals. In one trial, MK677 increased serum osteocalcin levels by 30% leading to improved gait speed, reduce numbers of falls, and a trend toward independent living in elderly test participants[5].
Of all of the peptide ghrelin analogues, Ipamorelin has the most profound effects on bone strength and density. Research shows that Ipamorelin can not only halt pathological bone loss, but can actually reverse it. Studies in rats show that Ipamorelin leads to a four-fold increase in bone formation and increase bone mineral density[6], [7].
In the end, there appears to be almost identical impact on bone strength and mineralization from MK677 vs Ipamorelin. Hopefully future research will unveil precisely why these ghrelin agonists have such profound impact on bone because not all ghrelin agonists demonstrate this effect. Even ghrelin itself has far more limited associations with bone health.
According to Dr. Conpinschi of the Free University of Belgium and an expert in sleep, the impact that MK677 has on sleep quality may actually be part of the reason that compound has been found to have neuroprotective effects. Beyond its ability to increase IGF-1 levels (discussed later), MK677 may be useful in thwarting both the normal effects of aging on the brain as well as pathological changes due to disease all because it improves sleep quality. In the realm of sleep, the battle between MK677 vs Ipamorelin tilts heavily toward MK677[8].
All GH secretagogues increase IGF-1 levels, but MK677 appears to be particularly adept at this, suggesting that it may be increasing IGF-1 levels in ways that extend beyond its impact on GH levels. Trials looking that ability of MK677 to reverse AD have been disappointing, but this is likely because the accumulation of amyloid beta has already had serious negative impact by the time the brain reaches AD. More encouraging research in mice indicates that MK677 administration over a lifetime can reduce amyloid beta buildup and that this does, in fact, decrease neuron and synapse loss. This suggests that MK677 may be a useful AD preventative and there is currently research to assess where it may be particularly useful in preventing AD in those who are genetically predisposed to the disease[9].
MK677 vs Ipamorelin
MK677, also known as Ibuatmoren and Oratrope, is an orally active, non-peptide, selective agonist of the ghrelin receptor. MK677 shares no structural similarities with ghrelin and therefore no structural similarities with Ipamorelin. Research shows that MK677 increases the secretion of growth hormone (GH) and insulin-like growth factor-1 (IGF-1) without affecting cortisol levels. It is currently under investigation for the treatment of growth hormone deficiency, muscle wasting, bone wasting, and appetite stimulation. MK677 has a long half-life and once-daily dosing in most trial settings.
Ipamorelin is a peptide analogue of ghrelin that stimulates the secretion of GH. It is among the most selective of ghrelin analogs with research revealing no effect on ACTH, prolactin, follicle-stimulating hormone, luteinizing hormone, thyroid stimulating hormone, or cortisol levels. Ipamorelin has been investigated in the treatment of GH deficiency, muscle wasting, and post-surgical ileus. It has also been the subject of numerous clinical trials for its ability to increase bone strength and mineralization.
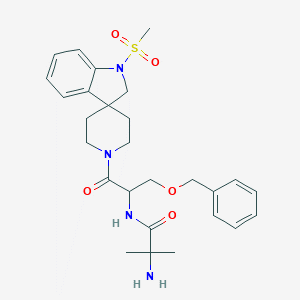
MK677
Molecular Formula: C27H36N4O5SMolecular Weight: 528.7 g/mol
PubChem CID: 9939050
Synonyms: MK-0677, Oratrope, Ibutamoren
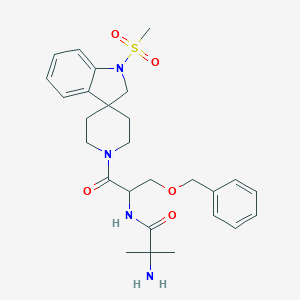
Source: PubChem
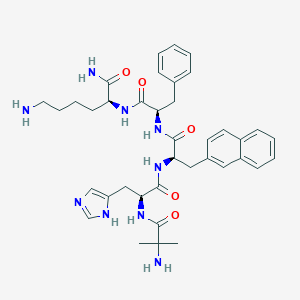
Ipamorelin
Amino Acids: Aib-His-D-2Nal-D-Phe-LysMolecular Formula: C38H49N9O5
Molecular Weight: 711.868 g/mol
PubChem CID: 9831659

Source: PubChem
MK677 vs Ipamorelin: Peptides and SARMs
Ipamorelin is a peptide. It is made up of amino acids and is based off of the naturally occurring ghrelin peptide found in mammals. MK677 is something else entirely. MK677 is often grouped with the selective androgen receptor modulators (SARMs) because it doesn’t fit neatly into any category. MK6767 isn’t a SARM though and it isn’t a peptide. It is a complex synthetic propenamide derivative that definitely fits into the category of growth hormone secretagogues[1].It is interesting that MK677 and Ipamorelin are so different because the effects these compounds have at the ghrelin receptor are very similar. Both bind to the ghrelin/growth hormone secretagogue receptor to boost GH release. Both also maintain the normal, pulsatile patterns of GH fluctuation. They both also have high degrees of specificity and therefore very few side effects.
Oddly, the fact that MK677 isn’t a SARM is of massive benefit. SARMs usually impact natural androgen production and can lower testosterone production. They certainly have their place in the clinical setting, but SARMs must be carefully administered to avoid side effects. Neither MK677 nor Ipamorelin has this requirement. There is no evidence that either molecule needs to be cycled to prevent tachyphylaxis (a loss of efficacy usually due to the down regulation of receptors in the setting of high stimulation).
MK677 vs Ipamorelin: Somatopause and Body Composition
Growth hormone secretion declines as a result of aging. Though this is a natural process, it should not be confused with a beneficial process. The loss of GH secretion with age is the reason we all lose muscle mass and accumulate fat mass over time. It is also part of the reason we experience bone density loss with age and can explain some of the sleep changes and cognitive changes that occur with age.Overcoming somatopause is a hot research topic. Studies suggest that stabilizing the GH axis produces a number of benefits with age including enhanced immunity, increase muscle strength, and improve cognition. While body composition may not seem like an important consideration with age, it is actually critical to health and wellbeing. Increased muscle strength helps to prevent things like slips, trips, and falls that become more common with age. Additional evidence suggests that elevated GH levels can help to reduce cardiac risk as well by driving down fat levels and the associated increases in triglycerides and cholesterol levels that come with high body fat content. It is worth noting too that fat is a source of inflammation that has been linked to diabetes and other inflammatory diseases. There is good reason to believe that reduced fat mass can help to prevent diabetes and even conditions like rheumatoid arthritis[2]. Inflammation is also a component of cardiac disease, so reducing total body inflammation may be just one of several mechanisms by which elevated GH levels help to thwart heart disease.
Both MK677 and Ipamorelin are under study for their ability to halt or even reverse some aspects of somatopause. MK677 is of particular interest due to its ease of administration. Whereas Ipamorelin is only active when injected, MK677 is highly effective when taken by mouth.
MK677 vs Ipamorelin: The Special Case of Bone Density
Given their drastic differences in chemical structure, it seems more than a little odd that MK677 and Ipamorelin have such similar effects on the body. This oddness is only further increased by research demonstrating that both peptides have a profound effect on bone density and mineralization.MK677 significantly increases both bone deposition and resorption, leading to increased bone remodeling[3], [4]. This can, when properly controlled, lead to increased bone strength and resistance to fracture. Pairing MK677 with physical therapy leads to increased bone density and decreased risk of hip fracture in elderly individuals. In one trial, MK677 increased serum osteocalcin levels by 30% leading to improved gait speed, reduce numbers of falls, and a trend toward independent living in elderly test participants[5].
Of all of the peptide ghrelin analogues, Ipamorelin has the most profound effects on bone strength and density. Research shows that Ipamorelin can not only halt pathological bone loss, but can actually reverse it. Studies in rats show that Ipamorelin leads to a four-fold increase in bone formation and increase bone mineral density[6], [7].
In the end, there appears to be almost identical impact on bone strength and mineralization from MK677 vs Ipamorelin. Hopefully future research will unveil precisely why these ghrelin agonists have such profound impact on bone because not all ghrelin agonists demonstrate this effect. Even ghrelin itself has far more limited associations with bone health.
MK677 and Sleep
If there is one place that MK677 outshines Ipamorelin it is in the realm of sleep. While Ipamorelin has definitely been associated with beneficial alterations in sleep quality, the magnitude of these effects pales in comparison to MK677. Research shows that MK677 has more profound sleep effects than any of the growth hormone releasing peptides. MK677 increases REM and stage 4 sleep dramatically and has been shown to decrease REM latency as well. Stage 4 sleep is generally considered to be the time when sleep is most restful, so increasing this stage of sleep should benefit feelings of well-being and being fresh in the morning. It likely also impacts things like wound healing and memory consolidation.According to Dr. Conpinschi of the Free University of Belgium and an expert in sleep, the impact that MK677 has on sleep quality may actually be part of the reason that compound has been found to have neuroprotective effects. Beyond its ability to increase IGF-1 levels (discussed later), MK677 may be useful in thwarting both the normal effects of aging on the brain as well as pathological changes due to disease all because it improves sleep quality. In the realm of sleep, the battle between MK677 vs Ipamorelin tilts heavily toward MK677[8].
Ipamorelin and Diabetes
Ipamorelin has been shown in animal studies to potentiate the release of insulin. This is thought to be an indirect result of stimulating the calcium channel of pancreatic islet cells where insulin is made and stored[2]. MK677 appears to have little to no effect on insulin release, suggesting that it does not interact with the calcium channel. When comparing MK677 vs Ipamorelin, the latter is clearly the better choice for impacting insulin secretion and researching potential mechanisms for stimulating the pancreas.MK677 vs Ipamorelin: IGF-1
GH and insulin-like growth factor-1 (IGF-1) levels rise and fall in pretty close correlation. IGF-1 is an important hormone in the pathway that clears amyloid beta from the central nervous system. Research indicates that IGF-1 levels are lower in patients with Alzheimer’s disease (AD), so raising these levels could be important in preventing or even treating AD.All GH secretagogues increase IGF-1 levels, but MK677 appears to be particularly adept at this, suggesting that it may be increasing IGF-1 levels in ways that extend beyond its impact on GH levels. Trials looking that ability of MK677 to reverse AD have been disappointing, but this is likely because the accumulation of amyloid beta has already had serious negative impact by the time the brain reaches AD. More encouraging research in mice indicates that MK677 administration over a lifetime can reduce amyloid beta buildup and that this does, in fact, decrease neuron and synapse loss. This suggests that MK677 may be a useful AD preventative and there is currently research to assess where it may be particularly useful in preventing AD in those who are genetically predisposed to the disease[9].